Mr. Y Case Study
This is a case study of an older gentleman who sustained a transtibial amputation following a motorbike accident in the summer of 2020 during the Covid pandemic.
SUMMARY
Private prosthetic provision is not uncommon following traumatic accidents involving limb amputation. However, NHS options are usually explored in order to minimise costs. During the Covid pandemic, the NHS struggled to provide a full prosthetic and rehabilitation service. Despite a few challenges along the way, Dorset Orthopaedic were able to support this gentleman to achieve his goals of walking again and riding his trike.
THE INDIVIDUAL
Mr Y was riding his motorbike when he was involved in a head on collision with a car driven by a young man. As a result, he sustained significant injuries to his right leg and was airlifted to his local trauma centre where he underwent a transtibial amputation.
Prior to the accident, Mr Y had been working as a part time commercial driver in his early seventies. He enjoyed walking his dog, gardening and DIY as well as riding his motorbike socially.
INITIAL ASSESSMENT AND PROGRESS
Mr Y was sent to Dorset Orthopaedic by his case manager as he was unable to be seen in his local NHS centre until the December of that year. He was first assessed in September 2020 and immediate plans were made to provide him with a prosthesis and with rehabilitation. Prosthetic fitting was challenging due to the knee on his amputated side being arthritic. This meant that it was sensitive around some of the areas where bodyweight would be taken. Having not taking any weight through this joint for a few months and then starting to walk again also meant that the knee became quite sore for a few weeks until it settled down.
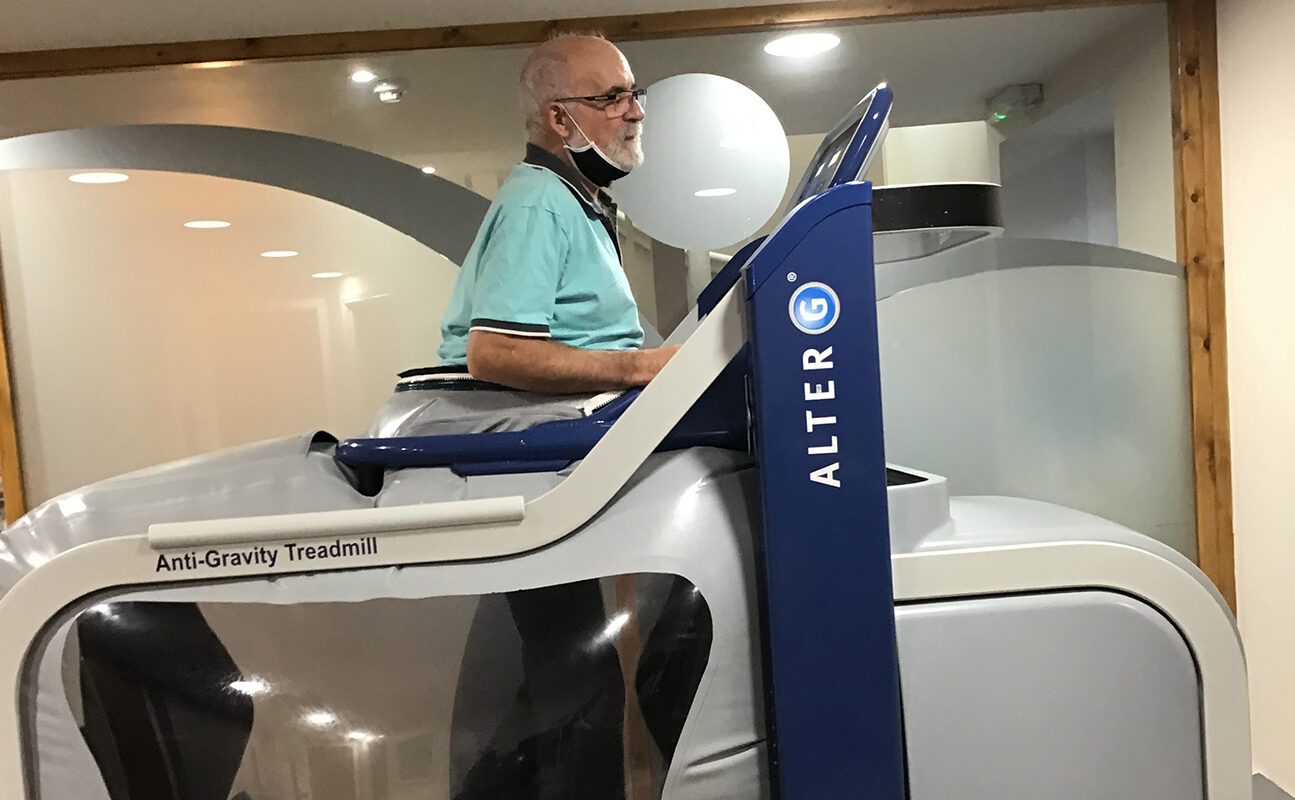
His rehabilitation sessions were quite intense with a variety of activities each time undertaken. These included specific strengthening, core and balance work, acupuncture to the right knee, sessions on the Alter G anti-gravity treadmill and outdoor walks.
Mr Y’s rehabilitation did not go smoothly and prior to his last two rehab days, he developed pain in the right shoulder and arm just before Christmas which was most likely due to prolonged use of walking aids. Mr Y and everybody involved in his care were rightly frustrated by this setback, particularly as the second wave of Covid then took a hold and Mr Y had to wait for investigations in a significant amount of pain. At this point he was using crutches, but was unable to bear weight on his left arm due to pain and almost complete loss of hand function. A pair of gutter crutches allowed some limited walking around the house during this time.
Unfortunately, he was never diagnosed with a reason for his left arm pain and loss of hand function. Carpal tunnel surgery was performed with limited change in the hand function and visits to a local physiotherapist were partly helpful. Over a few months, his pain settled and some hand function returned to enable him to recommence with us.
When a patient starts rehabilitation with us, we develop a problem list and set goals for them to work towards. Most patients state their goal is to walk again and hence we list those factors that are hindering them from achieving this. In Mr Y’s case, his problems were as follows:
Problem List
- Weak musculature both lower limbs but especially the right side
- Poor balance, dependent on stick for support
- Stump pain (scoring 6/10)
- Phantom limb pain – crushing pain in foot (scoring 9/10)
- Right knee pain (scoring 7/10) for a few paces on starting to walk
- Reduced cardiovascular capacity, managing 80m over a two-minute walk
- Altered gait pattern with longer stride on the right side one stick and managing half mile
- Reduced core strength – unable to sit up from supine position
- Not engaging in previously enjoyable recreation, such as DIY and motorcycling
Goals were then set to target each of the problems with the aim of walking largely unaided. We also take a number of outcome measures to demonstrate where progress is being made.
Outcome Measures
Objective measures demonstrate improvements in speed and agility when changing direction.
Objective Measures |
11/11/20 |
19/05/21 |
02/07/21 |
Timed up and go – a brief mobility timed test |
11.4s |
8.5s |
6.16s |
2 Minute Walk – distance walked over 2 mins |
80m over 2 mins |
125m over 2 mins |
132m over 2 mins |
4 Square Step Test – a brief mobility timed test |
17.5s |
9.78s |
Subjective measures inform us how the patient feels he is doing in respect of his functional ability, wellbeing and pain.
Subjective Measures |
11/11/20 |
19/05/21 |
02/07/21 |
Health and wellbeing score |
65% |
90% |
|
LCI-5 – a functional ability score |
40 |
56 |
|
Pain – stump |
6 |
0 (occasional stabs) |
5 |
Pain – phantom |
9 |
9 daily |
7 |
Pain – right knee |
7 |
2 |
0 |
Confidence in foot |
70% |
90% |
90% |
Perception of gait normality |
30% |
90% |
90% |
We usually advise amputees that they should be fairly competent walkers by the end of a year, with some further gains in the following year. Mr Y achieved his goals within the year and is now enjoying life again with his wife and dog. He has not returned to work but is considering some longer motorcycle holidays in the near future.