
Mr X Case Study
An elective transtibial amputee needing to return to frontline emergency duties
SUMMARY
Occasionally, traumatic injuries fail to heal and result in an elective amputation down the line. This is a case of a 37 year-old male who sustained lower limb fractures as a result of a motorbike accident. These fractures did not heal despite multiple surgeries including external and internal metalwork. Mr X was able to walk with crutches with the metalwork in situ but was keen to return to frontline duties and elected to have a transtibial amputation to enable him to move forward. He is currently undergoing rehabilitation with us and, at the six-month stage, is beginning to commence impact activities. This case study is an example of how we support primary elective amputees through the rehabilitation process from beginning to end.
THE INDIVIDUAL
Mr X was an active 35-year-old at the time of his injury in September 2018. He enjoyed time with his three young boys, jogging a few miles and an active, frontline full-time career which required a moderate level of fitness. Since the accident, he was able to walk approximately half an hour on crutches outdoors at a slow pace. Swelling of the leg was uncomfortable and he had gained over four stone. The various surgeries on his leg had resulted in significant scarring as can be seen below.

INITIAL ASSESSMENT AND PROGRESS
Mr X was first seen at Dorset Orthopaedic prior to his amputation for an initial assessment. We were able to talk to him openly about what to expect in the weeks following amputation and what kind of progress we could expect over time. He was able to see examples of the kind of prosthetic that could be provided and talk with another amputee. Some exercises were provided for pre-habilitation purposes.
At around two weeks following the amputation surgery, Mr X was able to drive himself to clinic to commence rehabilitation using an early walking aid known as the PPAM aid. This enabled early weight bearing through the limb which helped to reduce swelling, keep the tissues of the residual limb mobile and activate walking muscles appropriately. He was able to attend a number of times each week as funds were secured early via his case manager. Physiotherapy also included exercise to work on strengthening the muscles of the remaining leg and general fitness.
At six weeks, permission was sought and granted from his consultant to commence fabrication of a bespoke prosthetic leg. Mr X was then able to continue his walking safely at home, initially using crutches and progressing onto independent unaided walking. Some caution was required as the end of the residual limb did not have any sensation, hence Mr X would not have been aware if there was any rubbing or discomfort. Frequent skin checks are needed in this case to avoid skin breakdown.
Over the following weeks, Mr X attended Dorset Orthopaedic regularly, both for rehabilitation with physiotherapy, and also for further prosthetic sockets to be made as shrinkage in the limb occurred. Despite the pandemic, we have been able to progress rehabilitation in a safe way, using outside areas for exercise as much as possible and re-introducing Mr X to activities such as ball skills, uneven terrain and early jogging on the Alter G anti-gravity treadmill. He is now at the stage where we are introducing some impact into his regime in preparation for commencing jogging again. This requires developing power in the remaining muscles of the leg to compensate especially for the lack of calf muscle. Increasing the level of impact also means that the residual limb will experience more pressure inside the socket which could cause skin issues and hence progress needs to be graduated to ensure this doesn’t happen.
During his rehabilitation period, Mr X has also been on a phased return to work programme and now works full time in the training department where he is on his feet most of the day. His employers have allowed him to leave early once a week in order to continue his rehabilitation at Dorset Orthopaedic and to attend for full rehabilitation weeks. We have estimated that he will require four such intensive weeks during the year to achieve his goals and will be working alongside a local personal trainer in the interim now that the pandemic closures are coming to an end.
OUTCOME MEASURES
Whilst short and long term goals are important, outcome measures can be useful indicators of progress. In Mr X’s case, his short term goal was to walk unaided and his long term goal was to be able to regain a moderate level of fitness in order to pass a Bleep test, which involves running at a set pace between markers at slow to moderate pace over a number of minutes.
During his first intensive rehabilitation period, we took the following outcome measures:
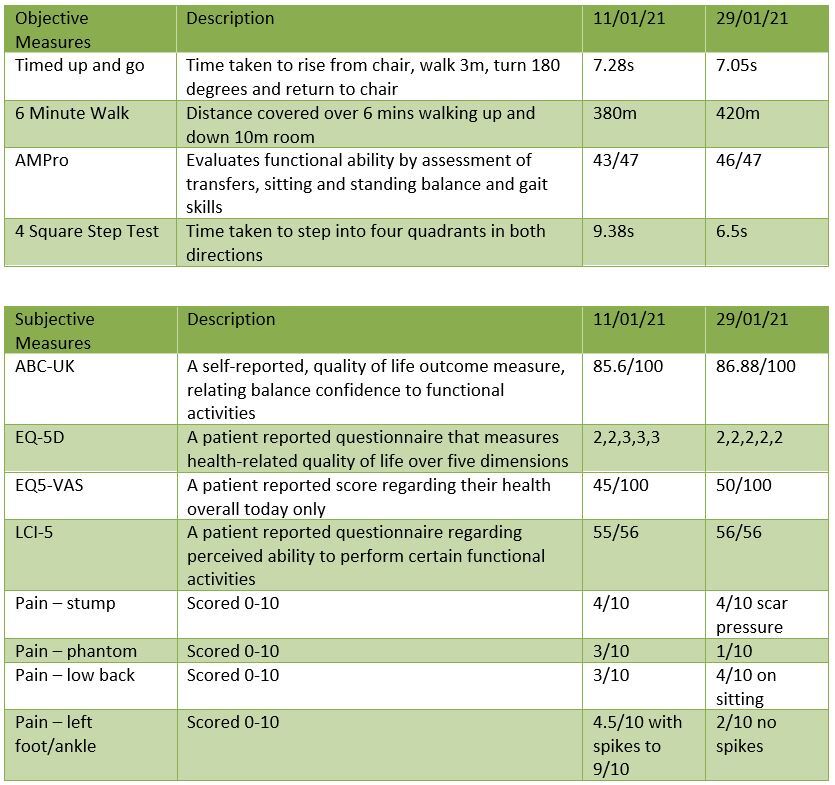
In general, there have been improvements over this two-week period in both speed, agility and functional measures. Pain has improved in the phantom limb and the left ankle but has worsened in the low back a little. Some attention will be paid to this in his next week’s rehab period which is scheduled for the end of April.
SUMMARY
The aim of a comprehensive rehabilitation programme is to restore an optimum quality of life for the individual, returning to previous work and leisure activities if they are able, and exploring new options for them in order to have an active and fulfilling life. We have been able to support Mr X through his initial rehabilitation and hope to work with him throughout the year in order to achieve his long term goals.